Why Archaeologists Should Care: The Bioarchaeology of Care
by Bill Evans III, Anthropology

Bioarchaeology is a subset of archaeology that focuses on the study of past persons and peoples through human remains, usually skeletonized. In bioarchaeology, the topic of disability has increased in popularity in the last few decades. Related to this trend of researching disability, new developments in theory appeared. One framework has appeared in numerous case studies over the last decade or so: the bioarchaeology of care. In this framework, researchers follow a four-step program to interpret cases of disability and care in the archaeological record. The four stages involve diagnosing disease, assessing disability, constructing a model of care, and interpreting the previous steps with ideas of collective and individual agency. The broad number of inputs and interpretative aspects allow researchers to reach more complex conclusions. In a noted case study, the framework was applied to an investigation of a plausibly quadriplegic adult male in Neolithic Vietnam, and this provided deeper insights into both his life and the lives of those around him. The bioarchaeology of care provides researchers with the theory to conclude a more detailed understanding of past persons’ and peoples’ lived experiences.
bioarchaeology, archaeology, bioarchaeology of care, care, disability
Introduction
Within the broader field of archaeology, bioarchaeologists study human remains and skeletons to interpret behaviors and health of past persons and peoples. This analysis often involves linking theory, data, researchers, and a healthy amount of guesswork. Although absolutes are not always possible, this does not stop bioarchaeologists from positing theories and reaching conclusions about human remains to inform archaeological research. This method guides researchers to remain flexible while also developing frameworks to follow for interpretation.
Bioarchaeologists often interpret past persons’ wellbeing and ills. An important condition seen in the archaeological record is disability. Disability is a human experience and common for humans to exhibit1. The World Health Organization, the United Nations agency responsible for investigating global healthcare, estimates that 1.3 billion persons experience significant disability today. The organization defines disability as the interaction of a health condition that negatively impacts wellbeing with personal and environmental compounds. Evidence of the widespread nature of disability demonstrates the importance and relevance of this issue.
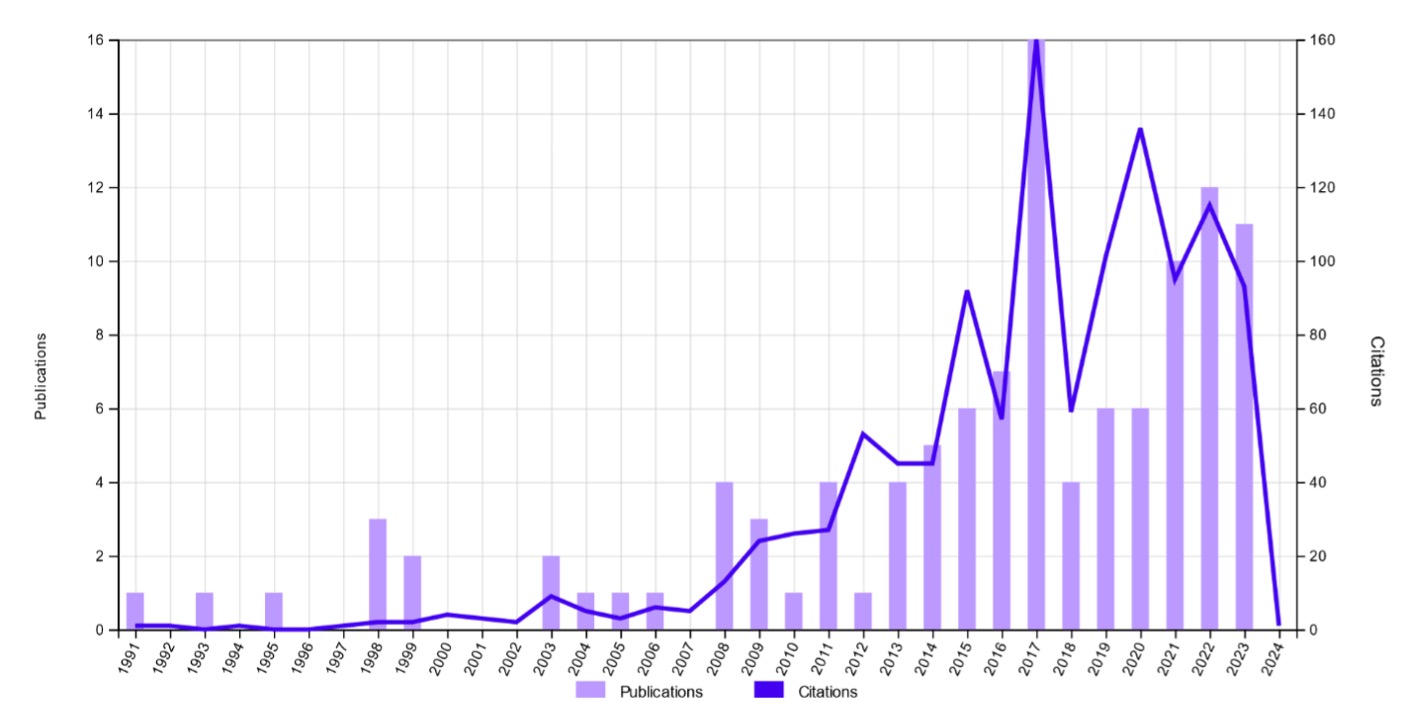
The topic of disability in archaeological research has grown exponentially in the past few decades. A citation report from the online database Web of Scienceshows citations and publications with the keyword “disability” from archaeological sources peaked in 2017 with a count of 180 and 16, respectively (Fig. 1). Of important note, the data for 2024 should be ignored since this query was run in early January of 2024 and represents incomplete data. Since the topic of disability has become increasingly researched and reported in archaeological research, it calls for investigation into the theory that drives this trend and its potential ramifications.
Fig. 1: Citation and publication report for “disability” from archaeological sources on the Web of Sciencedatabase2.
Inception of the Bioarchaeology of Care
Investigating disability in bioarchaeology is like any other archaeological inquiry and thus requires proper theory and framework. One proposed framework has been used in various case studies over the past decade or so: the bioarchaeology of care. First published by Drs. Lorna Tilley and Marc Oxenham in 2011, this framework allows for an interpretation of disability within larger cultural and communal responses to a person’s suffering3. This framework represents an important development in bioarchaeological theory. It broadens the typical application of theory to disease and disability, and the diverse number of inputs into the framework (agency, society, level of care required, condition, modern medical literature, context, etc.) create more detailed and accurate conclusions about past persons and peoples.
In the opening paragraph of her dissertation, Tilley discussed the creation of the framework and detailed the need to properly understand the care given to persons with disability to document communal, cultural, and societal knowledge3. Her later work refined the framework and clarified its development4. The framework is twofold: it includes both conceptual and applied components to interpret caregiving practices related to care in the archaeological record. In any given community, ideas about health, disease, and care in response to afflicted persons are formulated by variables such as “cultural norms, values and belief systems; traditions; collective skills and experience; political, social and economic organisation; environmental variables; and access to resources”4. Disability, as defined by Tilley in her framework, is a temporary or long-term state characterized by bodily impairments that are associated with activity or participation restrictions. Meaning is assigned to this state simultaneously by a person with disability and their community. The combination of disability and a person’s natural and artificial setting creates a complex environment that makes this practice so informative.
Stages of the Bioarchaeology of Care
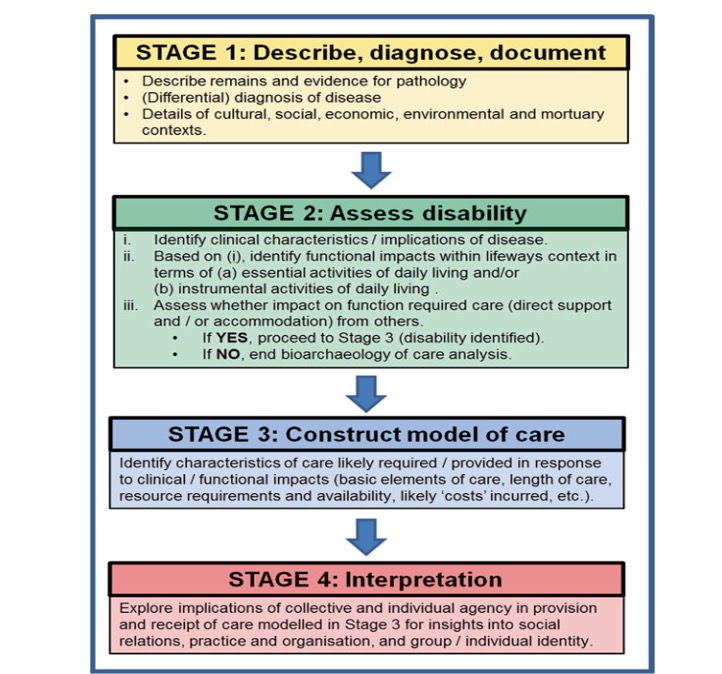
The framework is comprised of four stages that offer a step-by-step guide to investigate a person’s condition and the surrounding data contained in the archaeological record (Fig. 2). This analysis of care is qualitative and tailored to applications in case studies. The descriptions and figures aid researchers in flowing from one stage to the next in their analyses.
The first stage is to document a person, their conditions, and their context. This stage involves describing the state of human remains and the evidence for diagnosis. Their context would constitute the culture, society, economy, environment, and final resting place of the deceased. For example, a person could be buried outside of the community’s common cemetery. Tilley also stresses the need to devote attention to what qualifies as a person out of a set of humans remains (e.g., in the case of a mass burial)3. This step provides background data of the people surrounding the deceased.
The second stage establishes whether a case is valid for a provision of care. The data from stage one must be combined with modern medical literature to identify symptoms and prognosis. For example, a person could have suffered from arthritis but still be able to function day to day without assistance, and a case for provision of care would not exist. Much to the relief of researchers, many resources are easily accessible online detailing epidemiology, diagnostic criteria, comorbidities, treatment plans, etc. This stage also implores researchers to contemplate the impact of symptoms on a person’s ability to function in daily activities.
The third stage involves developing a model of care. Like the second stage, the third stage compounds on top of the previous results. This stage explores the duration and plasticity of care, effort, resources, and care efficacy (i.e., impact of the treatment) required for a person. For example, a person with severe, lifelong disability would require more resources, effort, and time to care for than a person with mild, short-term disability. An amalgamation of these features renders a plausible model of care received by a person. The first three stages follow a simple progression, but the fourth stage involves deeper interpretation.
The fourth stage is distinct enough that it warrants its own chapter in the text. This stage is unique in that it actively unpacks the entire process. In essence, it applies all the specifics learned back to the bigger picture and context from which the case originated. The first part of this stage involves group agency and identity. This stage guides researchers to describe the identity and motivations of the community. It can be helpful to think of the motivations of caregiving by describing the associated costs of treatment. For example, a people could have invested more resources into one person with disability than another due to their status as royalty. The second part of this stage involves individual agency and identity. It focuses on potential attitudes and views that a person could have carried about their treatment and situation. For example, it might be hard for a person with a painful disability to maintain a positive outlook on life, but this may be essential for survival. The end results of care are often dependent on the perspective and behavior of a recipient. A recipient, if they are able, has control over their treatment and attitudes. At minimum, a basic demographic profile should be created (e.g., sex and age) if possible. Combining these conclusions, researchers can make multiscalar analyses based on a single case of disability. Researchers can learn about both individuals and groups using a single case of disability and care. The fourth stage is arguably the broadest and most interpretive, but it also provides important conclusions from the data. In the author’s own words, the purpose of the fourth stage is “to bring the past to life”4.
Fig. 2: The stages of the bioarchaeology of care visualized and explained by its creator4.
Case Study of M9
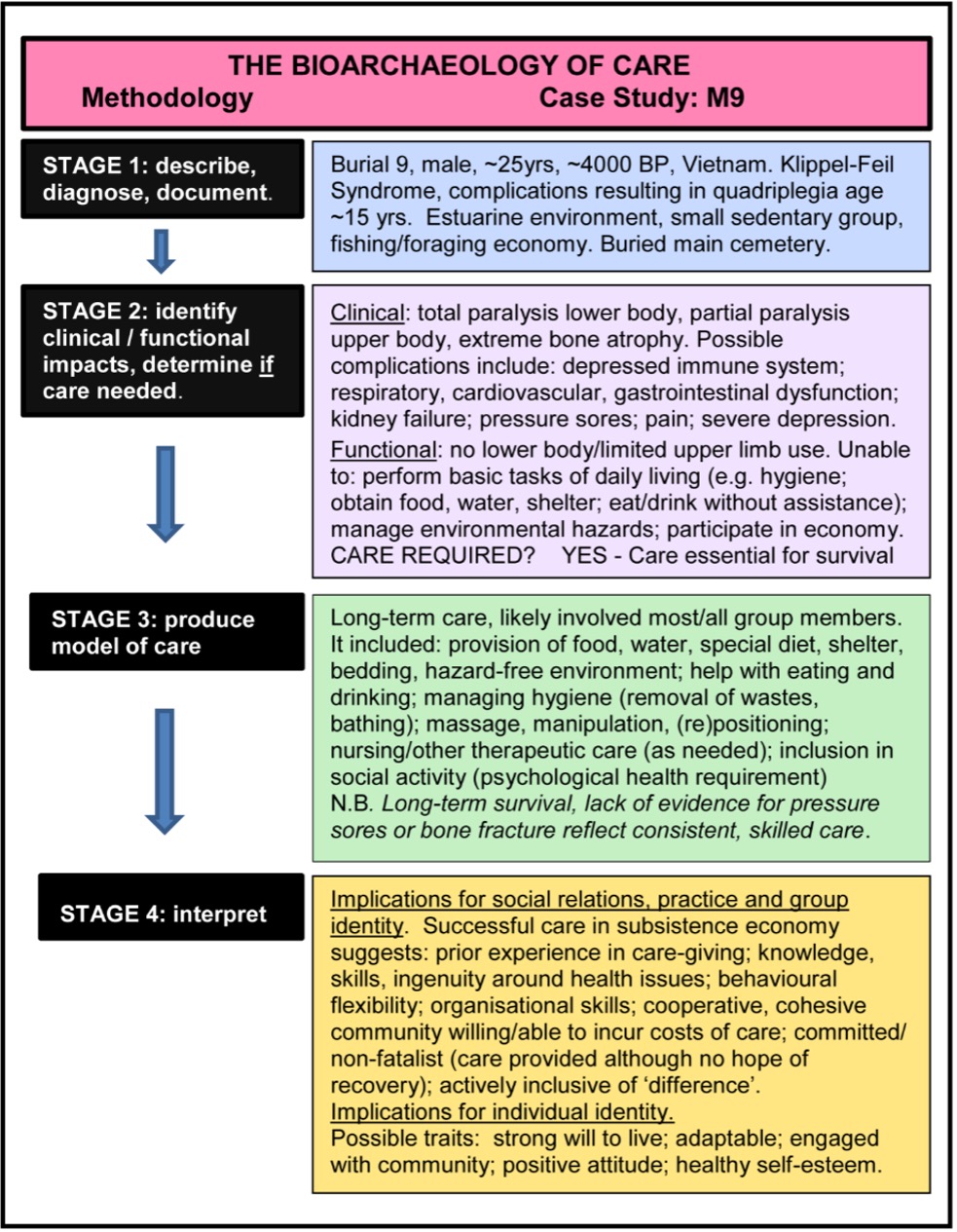
Since the inception of the framework, various publications have implemented it. Tilley and Oxenham wrote the first journal article on the subject in their investigation into the survival and eventual death of a plausibly quadriplegic adult male5. Man Bac Burial 9 (M9) lived in Neolithic Vietnam between approximately 3,700 and 4,000 years ago. This case study represents an important moment in the history of the bioarchaeology of care and data with which to demonstrate the framework (Fig. 3).
For the first stage, the researchers describe his disability and context. He was paralyzed from the waist down, and his upper body exhibited limited movement5. Although the extent of M9’s disability is not concrete, he was suffering from at best paraplegia and at worst quadriplegia from his youth into his third decade of life. The survival of this boy, and eventual development into manhood, represents a continuity of care and a plethora of resources, most notably time, from his community. The burial situation of M9 also contrasts with typical burials seen from the time: M9 was discovered lying north-south, on his right side, and flexed, contrasting the more standard east-west, supine, and extended burial. M9 exhibited atrophied lower and upper limbs, stiffness of the spine and neck, and degradation of the joint in his jaw. Previously, Oxenham proposed that M9 suffered from Klippel-Feil syndrome5. Clearly, his disability was extensive and took its toll on his body.
For the second stage, the researchers assess the implications of disability and the case for care. The extent of this condition guarantees that M9 would have depended on others for care, maintenance, and survival after becoming paralyzed3. M9 likely required care for simpler necessities like food, water, transportation, shelter, and dressing to more complex care like personal hygiene, supervision, and nursing. Consistent with modern medical findings, a case for care was necessary for M9.
For the third stage, the researchers develop a model of care. The combination of all this care constitutes an investment of resources from the community that lasted decades. The absence of pressure sores, evidenced by lack of skeletal infection, indicates at least a basic level of care. Lack of antemortem bone fracture reflects good quality of care when accounting for his porous and extremely gracile bones. M9 represents one of the earliest cases of long-term survival with severe disability.
For the fourth stage, the researchers postulate what these results mean for the suffering person and surrounding people. The effort of keeping M9 alive suggests that the community’s dichotomy of disease is nuanced and was not framed in terms of life-or-death outcomes. The survival of M9 could also indicate a high value of individual life and psychosocial support provided by caretakers. For the perspective of M9 as an actor with agency, he would have undergone at least the last decade of his life and late adolescence bedridden. This experience could have had detrimental effects to M9’s outlook on life and willingness to cooperate with care. The synthesis of all this information is an important theory-behind-care interpretation of this person and people.
Fig. 3: The bioarchaeology of care described in application to the case study of M9 by its creator7.
Limitations
Although the bioarchaeology of care is innovative and fruitful for research, it is not above criticism. Tilley herself addresses some of the framework’s limitations5. For starters, discussion surrounding disability in any context provokes strong opinions and feelings in many cultures. Research into disability often faces many barriers when seeking recognition and resources. Another limitation of this venue of research involves the power of interpretation of the archaeological record. A reflection of this is the problem of identifying specific research objectives in the subset of care and disability. The bioarchaeology of care explicitly states that, beyond the first stage, the investigation is based on logical inferences rather than presumptions. The framework also emphasizes the use of a standardized vocabulary for researchers to rely on when discussing individual and unique cases. Using analytical definitions and shared language, researchers can minimize criticisms of this framework and the research it produces.
Conclusion
In conclusion, the bioarchaeology of care represents the creation of an important framework in a previously underdeveloped region of analysis. Bioarchaeology, which can be rigid and empirical, stands to benefit from the infusion of holistic and interpretive techniques that this framework provides. Using the four stages of this framework, one cannot only talk about disability, one cannot only talk about care, one cannot only talk about a person, one cannot only talk about a people, but one can talk about the most detailed analyses of disability to date in bioarchaeology. In the case of M9, researchers were able to interpret much information beyond the diagnosis of M9’s paralysis. Although limitations of the framework exist, its creator has worked to refine the process through acknowledging barriers, emphasizing logic, and using standardized vocabulary. A more complete picture of human life is possible using a healthy amount of interpretation of care on multiple scales from individual to familial to communal to societal. This introduces an important conversation in bioarchaeology, and one that has the potential to improve understandings of persons’ and peoples’ lived experiences from the past.
References
- Disability. World Health Organization https://www.who.int/health-topics/disability (2024).
- Citation Report. Clarivate https://www.webofscience.com/wos/woscc/citation-report/7e9cb1bd-779b-4603-af19-4bddfcdd75ef-c4e08190 (2024).
- Tilley, L. A. Towards a bioarchaeology of care: A contextualized approach for identifying and interpreting health-related care provision in prehistory. (Australian National University, 2013).
- Tilley, L. Theory and Practice in the Bioarchaeology of Care. (Springer International Publishing, 2015).
- Tilley, L., & Oxenham, M. F. Survival against the odds: Modeling the social implications of care provision to seriously disabled individuals. Int. J. Paleopathol. 1, 35-42 (2011).
- Oxenham, M. F. et al. Paralysis and severe disability requiring intensive care in Neolithic Asia. Anthropol. Sci. 117, 107-112 (2009).
- Tilley, L. The bioarchaeology of care. Archaeol. Rec. 12, 39-41 (2012).
Acknowledgements: I would like to thank both Dr. Laurie Reitsema and Adam Kazmi individually. Dr. Reitsema taught us about the material and organization of arguments, while Adam provided feedback and mentorship.
Citation Style: Nature